
Anaesthesia for Robotic Surgery
Personalised anaesthetic care for the Illawarra
Your Anaesthesia for Robotic Surgery
Robotic-assisted surgery uses advanced technology to help your surgeon operate with greater precision. As your anaesthetist, I tailor my approach specifically for robotic procedures — including the steep positioning, longer operating times, and careful airway management these cases require.
Setting Your Expectations for a Calm Procedure
I look forward to looking after you on the day of your procedure.
Hopefully you have received information regarding your upcoming procedure. If you have, great. If not, feel free to read on.
Some people prefer as little information as possible; others find that a clear walkthrough reduces the stress of the unknown and gives them a chance to ask questions.
After all, we are trying to make a potentially stressful experience less so for you.
Your Pre-Surgical Roadmap
In the 24-48 Hours Before Your Operation
A few simple habits can make the whole experience smoother:
- Light exercise — a relaxed walk can help settle both mind and body.
- Nutritious meals — focus on good protein and sensible carbohydrates (pasta, rice, potatoes). This builds the energy stores you'll draw on while fasting.
- Immune preparation — think of this as a healthy "warm-up" for the normal surgical stress response.
- If you smoke — even stopping for 24 hours helps your lungs and circulation. Don't stress if quitting is difficult; every bit helps.
- Sleep — aim for a proper night's rest the night before.
- Fasting — follow the hospital's fasting instructions exactly; they're designed to keep you safe during the anaesthetic.
On the Day of Surgery
On arrival, you will be allocated a bed and an area to get changed.
If you are first on the day, the wait usually isn't very long before being called.
If you are booked later in the day, ask the nurse about "Sip to Send". Most anaesthetists, including myself, allow you to have a cup of water every hour until you are called to the theatre Holding Bay — a space outside the actual theatre room.
In the Holding Bay, it usually takes another 30-60 minutes before we actually go into the operating theatre. Numerous "pre-flight checks" have to be performed.
Going into Theatre
Once the theatre is prepared, most anaesthetists allow their assistant to walk you into the theatre to position you on the theatre bed. Mainly for two reasons:
- Despite being a large room, space is limited with all the sterile robotic equipment.
- The theatre bed is cold and sticky, despite our best efforts to warm it up. Re-adjusting your position is best done with your assistance on a "sticky" non-slip bed.
Monitoring equipment is then attached to you. An intravenous drip (IV cannula) is usually inserted in one arm or hand.
If you have a needle phobia, please let us know. Sometimes we can use gas to put you to sleep (without a mask) — some people prefer this to a needle.
Shortly after the drip is put in, you may feel like you have stepped into a "time warp". About 8-12 seconds later you will wake up in another room — the Recovery Room. The operation is over!
During the Operation — Positioning
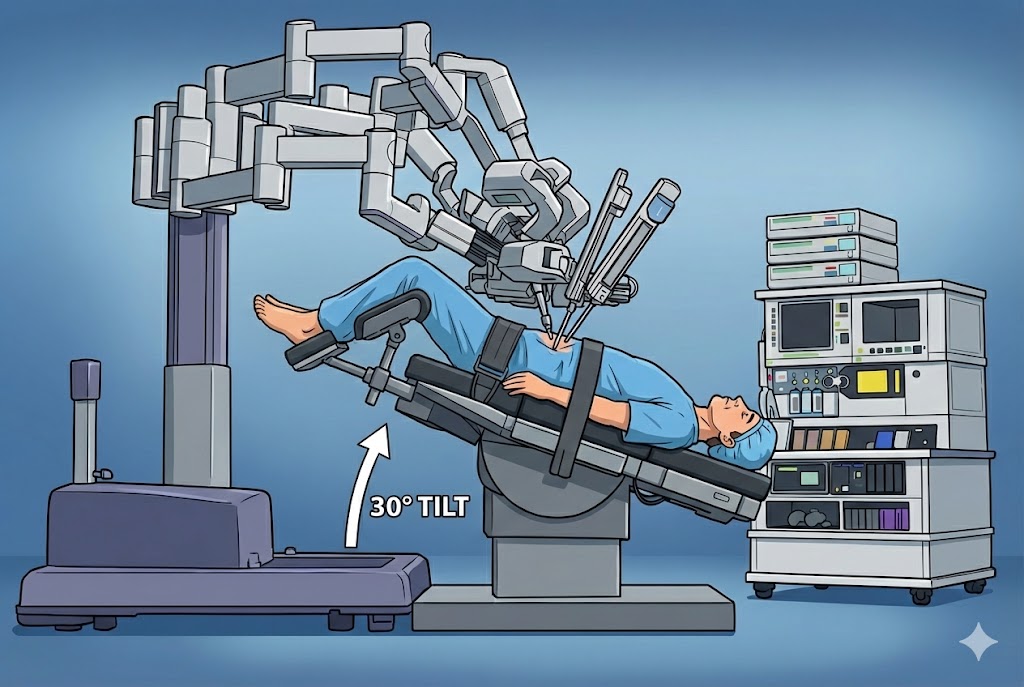
Position for Prostate or Bladder Surgery
Head-down (Trendelenburg) — usually closer to 30°
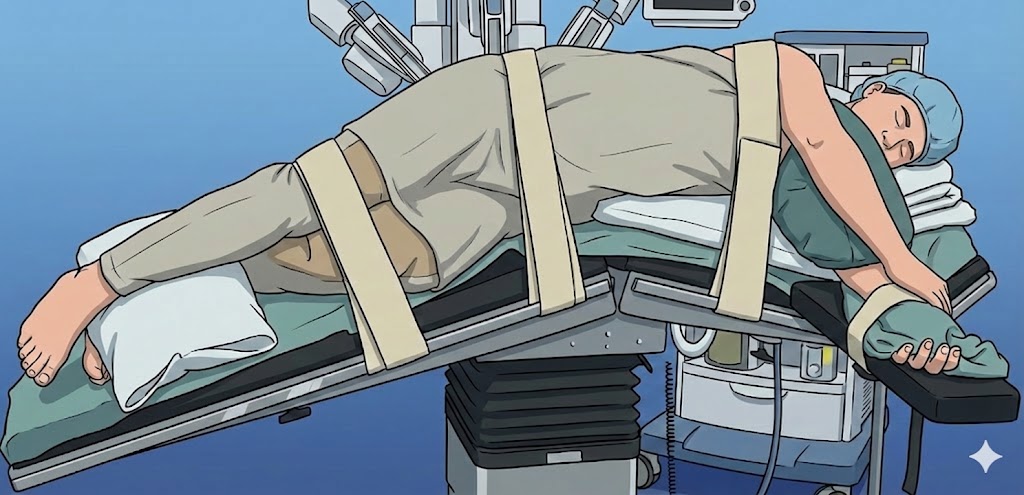
Position for Kidney Surgery
Arms padded, straps in place to prevent movement
- Arms are carefully wrapped and pressure pads are applied, as they are tucked in closely by your sides to avoid any damage to skin, muscles, and to avoid nerve compression.
- Stockings and calf compressors are placed on your legs to avoid pressure areas and keep the blood pumping in your legs to stop the formation of clots in leg veins.
- This is not a natural position to be in for 3-4 hours.
- Gravity causes blood to pool into the upper body and head.
- Gastric fluid can sometimes drain out of the mouth. Often a tube is placed into the stomach to limit this.
- Eyes need to be protected from gastric fluid — they are lubricated and covered with a fluid-proof dressing.
- The face, eyes, tongue, and brain can get "puffy" — much like your legs do when you've been on a long overseas flight.
- Numerous techniques are performed to limit this swelling. Monitors of brain swelling, for example, can be used.
In the Recovery Room
You are usually sitting upright, feeling groggy and disorientated, sometimes restless. This is completely normal. You have been given many drugs, and anywhere from 3-5 hours have passed performing your procedure.
You will have:
- A drip running through a vein
- Another cannula in the artery in your wrist, to take your blood pressure every time your heart beats
- A catheter into your bladder, taped to your leg
- Usually five small dressings on your abdomen
- Sometimes another tube (drain tube) in your abdomen
You are commonly nursed in a sitting position to allow blood to redistribute normally to the rest of your body.
During this time you may feel drowsy, disorientated, sometimes restless. Your vision may even be blurred, partially from lubricant used to protect the corneas. This may last for 2-3 hours, sometimes longer. This is all normal.
Nausea
Nausea is very common after most types of laparoscopic surgery. Most people feel nauseous for 24-48 hours, usually improving when your bowels open. You may require regular anti-nausea medication — I often chart it regularly.
If you have a history of motion sickness, please let me know. It increases your risk of nausea and vomiting after anaesthesia more than the average person. It can be stubborn to treat, but there are specific techniques and medications we can use to reduce the chance of it happening.
Pain
If you are in pain, ask the sisters in recovery — they have been instructed to give you pain relief until you are reasonably comfortable.
Catheter
The catheter in your bladder can feel uncomfortable for a while. That's normal. It's a foreign object, and your bladder instinctively wants to push it out, even though it's actually keeping your bladder empty. This sensation usually settles over the next few days as your body gets used to it.
On the Ward
Initially the abdominal wounds have local anaesthesia in them, which will wear off over 3-4 hours. This may occur when you have arrived on the ward.
Most painkillers are given regularly, but if you need more you can ask for "breakthrough pain" relief.
Keep in mind that everyone metabolises drugs differently. A painkiller that works for one person can sometimes not be as effective for another.
Rather than taking a large amount of one pain medicine, it's usually better to take small amounts of a few different ones. Each works on a different part of the pain pathway. This approach is called multi-modal analgesia, and it generally gives better relief with fewer side effects. So don't hesitate to ask if a different pain reliever might help.
Pain Killers (Analgesics)
Common ones I use are: Paracetamol, Diclofenac (Voltaren), Tapentadol (Palexia), Buprenorphine (Temgesic). Let me know if any cause you concern.
- These tend to have a lower incidence of constipation in most people.
- Temgesic can often make you feel drowsy, cloudy, or foggy in the head. Usually not unpleasantly so. Sometimes people feel they keep repeating themselves. That's ok.
- Palexia can sometimes make you feel dizzy.
- It's very common to feel light-headed the first time you get up or when you take a shower after surgery. Be mindful of this and take your time.
- It's usually not the pain medication causing it — it's the normal shifts in posture, blood pressure, and body fluids after an operation.
Bowel & Constipation
Most of the drugs used for pain relief can cause constipation. Constipation can also be reduced by maintaining your hydration, drinking plenty of fluid, and eating wisely (e.g. high fibre, green veggies, and cereals). Commonly a stool softener will be prescribed.
The bowel often goes on "holiday" after major surgery. It's completely normal for it to take 24 hours or longer before you open your bowels.
A few simple things can help wake it up:
- "Grazing" — instead of three big meals, try small amounts every 30-45 minutes or so.
- Chewing gum — this stimulates the gut by triggering the same nerves involved in digestion.
These small tricks nudge the bowel back into gear without overloading it.
If you have a drain in your abdomen, you can experience hiccups, belching, sometimes nausea. Once it comes out, your bowels are likely to only then start to wake.
At Home
Follow the pain relief information given to you:
- Regular Paracetamol (Panadol) for 4-5 days.
- You can add NSAIDs (non-steroidal anti-inflammatory drugs) like Diclofenac or Nurofen.
- Stronger drugs like Tapentadol can be taken when necessary — probably best taken at night time over the next 3-5 days, as this is when bruising and swelling around the wounds are at their peak.
I hope this has been helpful.
You're always welcome to send feedback by email or through my rooms. I'm continually working to make an unpleasant experience a little less unpleasant, and your feedback genuinely helps.
Frequently Asked Questions
When should I stop eating and drinking?
You must not eat any solid food for 8 hours before your arrival. Clear liquids may be permitted up to 4 hours before, but please adhere strictly to the specific fasting timeline provided by your surgeon to avoid cancellation.
What medications should be avoided?
Certain medications, particularly blood thinners, anti-inflammatories like Ibuprofen, and some herbal supplements can increase bleeding risks. You will receive a comprehensive list of what to pause and what to continue on the morning of surgery during your pre-op call.
Do I need someone to drive me home?
Yes. If you are receiving sedation or general anaesthesia, hospital regulations require a responsible adult to drive you home and stay with you for the first 24 hours. Taxis or ride-sharing services are not acceptable unless accompanied by a caregiver.
What should I wear on the day?
Choose loose, comfortable clothing that is easy to remove and put back on. Avoid jewellery, piercings, contact lenses, and heavy makeup. Wear flat, stable shoes to ensure your safety when walking post-procedure while still recovering from sedation.
How long is the typical recovery?
Recovery varies by procedure. You will transition from the Post-Anaesthesia Care Unit (PACU) once your vital signs are stable and pain is controlled. Your surgeon will provide specific post-operative milestones and activity restrictions before discharge.
Clinical Support & Inquiries
Your safety and peace of mind are our priority. If you have any medical concerns or require clarification on your pre-surgical expectations, please reach out.
Phone: (02) 4228 5055 | Email: iass@iass.net.au
Address: 409 Crown Street, Wollongong NSW 2500